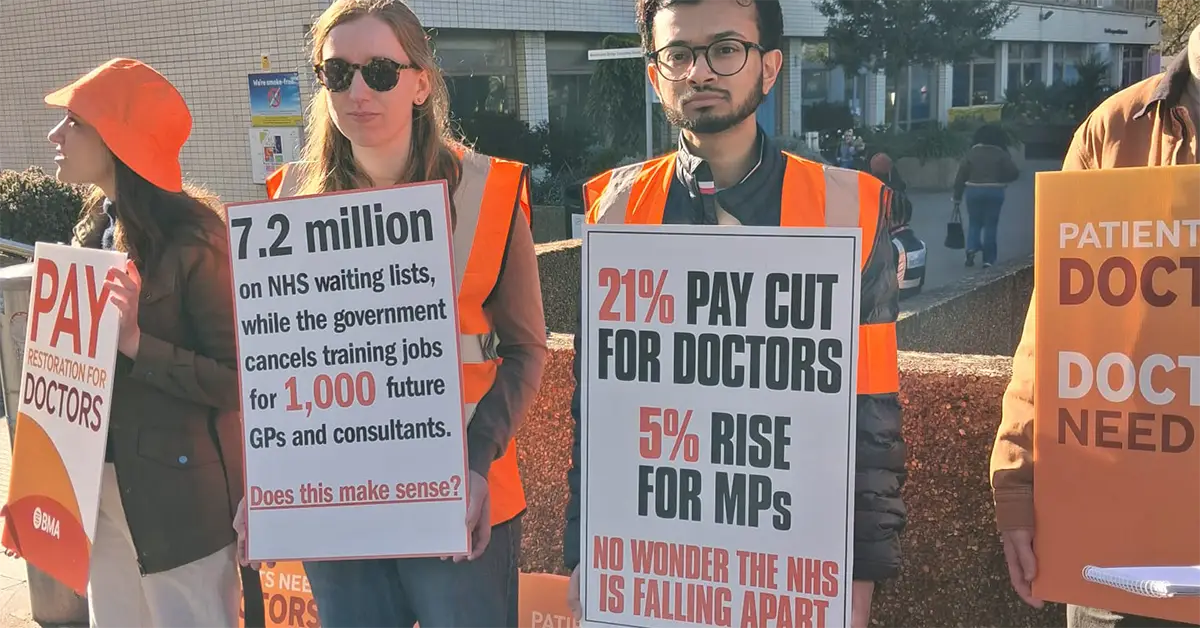
Resident doctors in England are now in their fifteenth round of strike action since 2023. The current six-day walkout is the longest in the dispute so far. They are striking over two connected issues: pay that has fallen by around 21 percent in real terms since 2008, and a jobs bottleneck so severe that 50,000 doctors are competing for fewer than 13,000 specialty training places.
Both problems come from years of underfunding. Both now confront a government that has chosen to treat the doctors as the problem.
The demands are clear. The BMA wants full pay restoration to 2008 levels, enough training posts to meet the NHS’s own workforce needs, and an end to a pay progression system the government can rewrite at will. The latest offer was a 3.5 percent rise this year, below retail price inflation, with the rest spread over three years and tied to productivity conditions. The BMA’s Resident Doctors Committee rejected it as a deal that, at best, barely treads water.
Health Secretary Wes Streeting then withdrew a promised 1,000 additional training places, saying the doctors had forfeited them by striking. Even that supposed concession was thin. Most of it came from promises the government had already made. The jobs issue remains one of the government’s weakest points, because it connects directly to staffing shortages, waiting lists and the daily reality of a service that cannot cope.
With 1,700 patients a day already waiting more than twelve hours in emergency departments, and a waiting list of 7.2 million, the government’s answer to a workforce crisis is to punish staff and patients alike.
Labour’s case does not hold up
Labour ministers keep insisting the doctors have already been offered enough. Streeting’s headline claim is that his package would have left resident doctors 35.2 percent better off than they were four years ago. That figure rolls together different increases across different years. It is meant to make the strike look like greed.
What it hides is the actual point at issue. Pay is still around 21 percent below its 2008 value in real terms. The cost of settling the dispute in full is £1.7 billion, less than one percent of the NHS’s total annual budget of £242 billion. The money exists. The question is what the government chooses to spend it on.
That question matters beyond the resident doctors’ dispute. Another cost-of-living squeeze is already taking shape. Prices remain high, rents are rising again, and workers across the economy are being told to settle for less. That creates the conditions for a broader fight, including in the NHS. Doctors are not asking for something exceptional. They are one section of workers refusing another round of managed decline.
As we have argued before, Streeting’s language of NHS reform covers a broader programme of restructuring. Cuts are rebadged as efficiency savings. Outsourcing to private providers expands. Public money continues to flow into corporate profit. Private firms cherry-pick the easiest work, while NHS staff deal with the complications, the emergency pressures and the staffing crisis.
This is not a temporary squeeze while the books are balanced. It is a political project to reshape the NHS and narrow what it is for. The doctors’ dispute sits squarely in its path.
The union bureaucracy is helping to isolate the strike
Other union leaders have not rushed to show solidarity. On the eve of the strike, senior figures from other health unions briefed the Guardian anonymously that the BMA was making their own deals harder to defend. One admitted the point directly: the doctors’ refusal to accept 3.5 percent was making the below-inflation settlements they had negotiated a much tougher sell.
Another complained that resident doctors themselves were leading the BMA negotiations rather than leaving it to professional negotiators. In plain terms, members who know what they are fighting for are harder to manage than officials who know what they are prepared to accept.
What neither source mentioned was that last year’s Agenda for Change settlement, which covers nurses, midwives, paramedics and most other NHS staff, was rejected in indicative ballots by Unison, Unite, GMB and the Royal College of Nursing. Those ballots were structured to exclude any mandate for industrial action.
The bureaucracy’s real problem with the doctors is not that they are negotiating badly. By refusing to lose quietly they expose the low ambitions of other health unions, whose leaders have put stable relations with the employer, and above all with a Labour government, ahead of their members’ interests.
Anyone in a hospital knows the pressure does not stop with doctors. Unsafe rotas, disappearing breaks. Nurses, healthcare assistants, physios, porters, domestics, admin staff and lab workers are all trying to hold together a service that is permanently overstretched.
As we noted last autumn, more than 40,000 nursing vacancies tell their own story about NHS pay. This year’s 3.3 percent Agenda for Change settlement does not come close to addressing that.
NHS workers need a coordinated struggle
The 2022–23 strike wave showed what was possible when NHS anger found collective expression. It also showed what the union leaderships did with that anger. They brokered below-inflation deals and channelled the energy behind a Labour government that is now deepening the same restructuring and privatisation drive it inherited from the Tories.
That is the setting in which Labour will try to make the argument sectional. Doctors are to be presented as the group that asked for too much, while everybody else accepts what is on offer. The obvious problem is that other NHS workers need more as well. Cutting the doctors down will not improve anybody else’s position. It will make it easier for the government to hold the line across the whole service.
That is also why some union leaderships are helping to make that case. The answer is to back the doctors, fight for more for every section, and push for a coordinated struggle across the whole NHS workforce.
Fifteen rounds of action over three years shows real determination. They also carry a warning. Ballot turnout has fallen from 77.5 percent in early 2023 to 52.5 percent in February 2026. Public support has fallen too, from majority backing in 2024 to around 30 percent by the end of last year. Repeated short strikes by a single group, without escalation and without the fight widening, tend to produce exactly that result. Workers get tired, the public grows impatient and the government can afford to wait it out.
Ministers are counting on that. The method has to change before the dispute is worn down further. A doctors’ fight has to become an NHS fight, and an NHS fight has to become a political problem the government cannot simply sit out.
Turn a doctors’ fight into an NHS fight
The lesson should be obvious by now, even if the unions have not acted on it. The government’s strategy is to divide the fight profession by profession and wait for each section to burn out on its own. Hospital workers should not repeat that mistake.
There should be joint meetings in every hospital. BMA, RCN, Unison, Unite and GMB members should meet together and argue through what common demands and common action would look like. Picket lines should be backed. Collections should be organised. Delegations should be built. Pressure should be put on the union leaderships to stop treating every dispute as a separate problem with a separate ceiling.
This is not just a trade union question. Governments always reach for the same argument: patients may suffer, so staff must accept what they are given. But patients already suffer every day from understaffing, delay and a service kept running through overtime and overwork.
The fight to defend the NHS cannot be won by any one group of workers alone. It needs a combined staff campaign. It also needs a wider mobilisation of patients, carers and community organisations that can turn an industrial dispute into a sustained political problem for a government running the service on the cheap.
That is why the fight for a new workers’ party matters. The doctors’ dispute needs a political force that can turn industrial solidarity into sustained pressure on the government. It needs one that is active in the workplaces and communities carrying the cost of this crisis, not one that appears only at election time.
The doctors are not asking for anything extravagant. They are trying to claw back what they have lost. In doing so, they are holding a line that every NHS worker has an interest in defending. The task now is to stop this fight being fenced off and worn down in isolation, and to use it to raise the wider question of pay, staffing and what the NHS is actually for.